
Advanced Cardiovascular Labs
1. Apolipoprotein B
Apo B is a direct measurement of all the atherogenic particles that a patient has (VLDL, IDL, LDL, and Lipo (a)) so it is the most accurate measurement of "bad" cholesterol. On the other hand, LDL cholesterol is an indirect measurement based on a calculation, so lab results can vary up to 30% . . . and LDL cannot even be calculated if the patient’s triglycerides are too high.
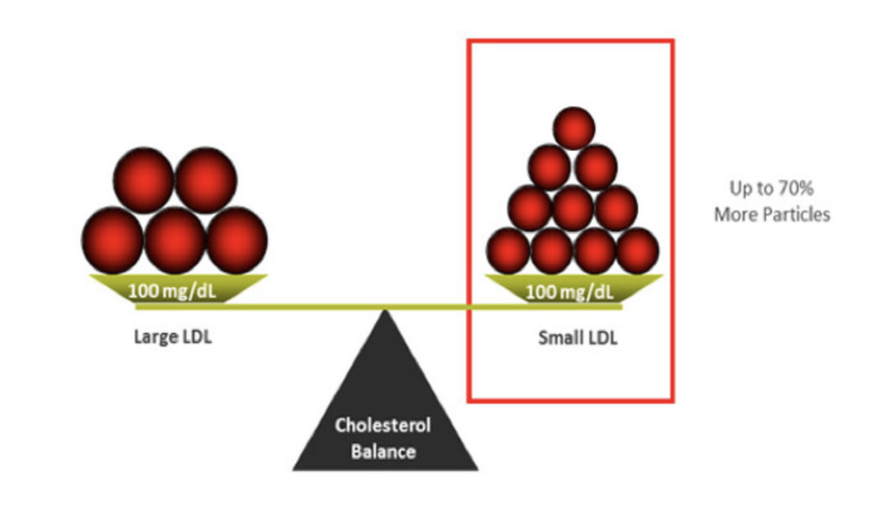
The slide below is an example of two different patients who have the same LDL cholesterol (100 mg/dL), but their Apo B is different. Think of cholesterol like traffic in your arteries. You could have either 5 cars (cholesterol particles) with 20 cholesterol passengers (like on the left) or you could have 10 cars (cholesterol particles) with 10 cholesterol passengers (like on the right). Either way you are transporting 100 passengers (100 mg/dL of LDL cholesterol). The more cars (particles) you have, the more traffic in your arteries and the higher the CV risk. A higher Apo B level reveals this CV risk, as demonstrated in the patient on the right. which was NOT identified by the level of LDL cholesterol.
The slide below is an example of two different patients who have the same LDL cholesterol (100 mg/dL), but their Apo B is different. Think of cholesterol like traffic in your arteries. You could have either 5 cars (cholesterol particles) with 20 cholesterol passengers (like on the left) or you could have 10 cars (cholesterol particles) with 10 cholesterol passengers (like on the right). Either way you are transporting 100 passengers (100 mg/dL of LDL cholesterol). The more cars (particles) you have, the more traffic in your arteries and the higher the CV risk. A higher Apo B level reveals this CV risk, as demonstrated in the patient on the right. which was NOT identified by the level of LDL cholesterol.
The ADA (American Diabetes Association), ACC (American College of Cardiology), and NLA (National Lipid Association) all endorse Apo B as superior to LDL-C for marking CV risk. There is no disputing the evidence:
Apo B is the single most significant and consistent lipid measurement to predict CHD risk. 5 It is a powerful marker of vascular disease and a better guide to the adequacy of therapy than any other lipid biomarker. 6
**CONCLUSION: Apo B should be used to assess CV risk, not LDL-C.
- In the Health Professionals Follow-Up Study, apo B was strongly associated with C-V risk, while LDL-C and non-HDL-C were NOT statistically significant. 11
- In the AMORIS study, apo B was shown to be a significant predictor of fatal heart attack in both men and women, but LDL-C was insignificant in women (and only modestly associated in men). 10
- In the EPIC study, LDL-C does not predict coronary artery disease (CAD) risk, but LDL particle number does (a surrogate marker of apo B). 1
- In the JUPITER trial, baseline LDL-C was not associated with CV events, but apo B was. 2
- In the AFCAPS/TexCaps study 12 and the LIPID study, 13 Apo B was shown to be a superior marker of CV risk than LDL-C.
- In the CARDIA study, Apo B was determined to be a better predictor of coronary artery calcium score than LDL-C. 3
- A large meta-analysis of twelve independent reports (including 233,455 subjects and 22,950 CV events) concluded that Apo B is the most potent marker of CV risk, LDL-C is the least, and non-HDL-C is intermediate. 7 Based on number of CVD events at 10 years, a treatment strategy that used Apo B instead of LDL-C would prevent 500,000 – 800,000 more CV events! 4 7
Apo B is the single most significant and consistent lipid measurement to predict CHD risk. 5 It is a powerful marker of vascular disease and a better guide to the adequacy of therapy than any other lipid biomarker. 6
**CONCLUSION: Apo B should be used to assess CV risk, not LDL-C.
How do you lower ApoB?
Diet, exercise, and weight loss can all help lower Apo B. Interestingly, exercise has not been shown to decrease LDL-C much, but it does lower Apo B, so it is certainly still lowering the atherogenic burden and benefiting the patient. 25
Statin cholesterol medications are typically very effective at lowering Apo B levels. Sometimes niacin or zetia are added onto therapy to further lower levels. In the higher risk patient, PCSK9 inhibitors might be used - these are extremely effective at lowering Apo B levels.
Diet, exercise, and weight loss can all help lower Apo B. Interestingly, exercise has not been shown to decrease LDL-C much, but it does lower Apo B, so it is certainly still lowering the atherogenic burden and benefiting the patient. 25
Statin cholesterol medications are typically very effective at lowering Apo B levels. Sometimes niacin or zetia are added onto therapy to further lower levels. In the higher risk patient, PCSK9 inhibitors might be used - these are extremely effective at lowering Apo B levels.
2. Lipoprotein (a)

Lipoprotein(a) is an inherited type of LDL cholesterol that accelerates the progression of atherosclerosis (plaque build up in the arteries). Also known as “sticky cholesterol,” it is a small, dense, highly inflammatory protein that has been shown to be an independent risk factor for early coronary artery disease (as acknowledged by the American Heart Association, American College of Cardiology, and European Atherosclerosis Society). Think of Lp(a) like a “FAST PASS” – it gets cholesterol into the lining of the artery quicker. In addition, elevated Lp(a) levels can also increase a patient’s propensity for developing blood clots.
Important facts about Lp(a)
- One in five people have high Lp(a) levels, and most of these people do not know they are at risk.
- The amount of Lp(a) your body makes is determined by genetics (you have to inherit the ability to produce it from one of your parents).
- 18% of patients with premature coronary artery disease (CAD) have elevated Lp(a). High Lp(a) is the strongest, single, inherited risk factor for early blockages in the heart and aortic stenosis (narrowing of the aortic valve opening in the heart).
- According to the Copenhagen data, as Lp(a) levels went up there was a consistent increase in the risk of a heart attack, starting at a level around 40-50 mg/dL. Each doubling of the level increased the CV risk an additional 20%.
- Lp(a) can raise the risk of cardiovascular disease by 200–400%. High levels of Lp(a) have been correlated with an increased risk of: coronary artery disease (CAD), stroke, peripheral vascular disease (PVD), abdominal aortic aneurysm (AAA), re-stenosis (after a stent), and retinal artery occlusion (obstruction of blood flow in the eyes).
Who should get tested for Lp(a)?
We believe everyone should find out as soon as possible if they carry this silent artery clogger. However, certain groups of people should absolutely ask for the test. These include:
We believe everyone should find out as soon as possible if they carry this silent artery clogger. However, certain groups of people should absolutely ask for the test. These include:
- People who have personally suffered a heart attack or stroke (especially without any other known risk factors).
- People who have a family member with early heart disease or stroke (men younger than 55 years of age and women less than 65 years of age)
- People who have family members (parents, siblings, children) with high Lp(a). If a parent has high Lp(a), the child has a 50% chance of inheriting it.
- People taking cholesterol medication who still have abnormal lipids. (It could be the LDL cholesterol in Lp(a) that is contributing to these elevations).
How can you lower Lp(a)?
Lowering Lp(a) has been shown to reduce CV risk by 70-75% but there is no prescription treatment available at this time that is indicated for lowering Lp(a). We are limited in effective therapies. Because of this, patients with elevated Lp(a) should be treated aggressively for all other CV risk factors (blood pressure, blood sugar, sleep apnea, poor diet, smoking, lack of exercise, etc.). Doing this can lower the patient’s risk of a heart attack or stroke even if they have high Lp(a).
Unfortunately, diet and exercise have no impact on lowering Lp(a) levels, and neither do statin cholesterol medications. A meta-analysis of over 29,000 patients showed that statin treatment does not mitigate the risk of Lp(a).
The most effective treatment we have now for lowering Lp(a) is high dose niacin (nicotinic acid), a form of vitamin B3. This vitamin can lower levels by about 25% (while also lowering LDL cholesterol, lowering triglycerides, improving particle size, and raising HDL cholesterol). The EAS advises 1-3g of niacin daily, but it can cause a side effect of flushing. Other than this irritating side effect, niacin has been used safely for decades.
In addition to niacin, we know estrogen can lower Lp(a) levels. Lp(a) levels do not change much during one’s lifetime unless you are a woman. During menopause Lp(a) levels go up as estrogen level decline. In post-menopausal women, a recent review demonstrated a powerful effect of hormone replacement therapy on Lp(a) levels. Data from the HERS trial confirms this. In this trial, 2,763 postmenopausal women with a history of heart disease were put on Prempro. Overall this trial showed that hormone replacement therapy (HRT) conferred no CV benefit, but in the subset of patients who had elevated Lp(a), HRT DID show a reduction in CV events! Take home message - HRT may be worth considering for women with high Lp(a).
Low dose aspirin has been shown to help lower levels of Lp(a). Aspirin may also benefit these patients by helping to combat the increased clotting risk from high Lp(a). So daily aspirin therapy may be worth considering in people with elevated Lp(a).
Lowering Lp(a) has been shown to reduce CV risk by 70-75% but there is no prescription treatment available at this time that is indicated for lowering Lp(a). We are limited in effective therapies. Because of this, patients with elevated Lp(a) should be treated aggressively for all other CV risk factors (blood pressure, blood sugar, sleep apnea, poor diet, smoking, lack of exercise, etc.). Doing this can lower the patient’s risk of a heart attack or stroke even if they have high Lp(a).
Unfortunately, diet and exercise have no impact on lowering Lp(a) levels, and neither do statin cholesterol medications. A meta-analysis of over 29,000 patients showed that statin treatment does not mitigate the risk of Lp(a).
The most effective treatment we have now for lowering Lp(a) is high dose niacin (nicotinic acid), a form of vitamin B3. This vitamin can lower levels by about 25% (while also lowering LDL cholesterol, lowering triglycerides, improving particle size, and raising HDL cholesterol). The EAS advises 1-3g of niacin daily, but it can cause a side effect of flushing. Other than this irritating side effect, niacin has been used safely for decades.
In addition to niacin, we know estrogen can lower Lp(a) levels. Lp(a) levels do not change much during one’s lifetime unless you are a woman. During menopause Lp(a) levels go up as estrogen level decline. In post-menopausal women, a recent review demonstrated a powerful effect of hormone replacement therapy on Lp(a) levels. Data from the HERS trial confirms this. In this trial, 2,763 postmenopausal women with a history of heart disease were put on Prempro. Overall this trial showed that hormone replacement therapy (HRT) conferred no CV benefit, but in the subset of patients who had elevated Lp(a), HRT DID show a reduction in CV events! Take home message - HRT may be worth considering for women with high Lp(a).
Low dose aspirin has been shown to help lower levels of Lp(a). Aspirin may also benefit these patients by helping to combat the increased clotting risk from high Lp(a). So daily aspirin therapy may be worth considering in people with elevated Lp(a).
3. Focused inflammatory panel (hs-CRP, LpPLA2, MPO)
Inflammation is ultimately the source of all cardiovascular (CV) disease, but it is also the driving force behind other serious illnesses like cancer, autoimmune disease, and even dementia. When the arteries are inflamed, cholesterol particles can “stick” and accumulate more easily into the arterial walls, eventually forming plaques that can cause a heart attack or stroke.
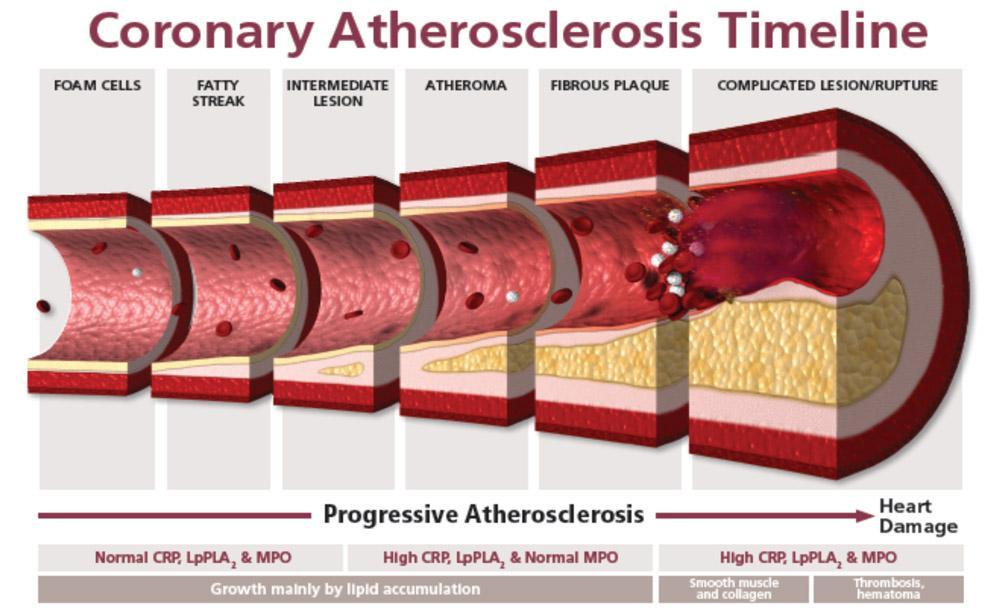
- In the earliest stages of atherosclerosis, inflammation biomarkers measured in the blood (hs-CRP, LpPLA2, and MPO) are normal.
- In the intermediate and later stages of atherosclerosis, hs-CRP is elevated.
- In the presence of active arterial wall plaque, LpPLA2 is increased.
- And in the presence of unstable plaque (that could easily rupture), MPO is increased.
a) hs-CRP (high sensitivity C-reactive protein)
C-reactive protein is an acute phase inflammatory plasma protein made by the liver, so it will rise in conjunction with systemic inflammation from many different sources. For this reason, the “high sensitivity” CRP test is necessary for detecting low levels of CRP that correlate more with endothelial (vascular) inflammation.
In general, if “high sensitivity” CRP is between 1-5 then it is more likely a marker of CV risk, but if it is over 10 then the elevation could be from an acute infection, a recent injury, or another non-cardiac source like autoimmune disease.
The hs-CRP biomarker should decline with effective disease management, so it can also provide independent prognostic information after initiating treatment (to help assess how well a patient is responding to lifestyle changes and statin medication).
We cannot discuss hs-CRP without acknowledging the results of the Jupiter Trial. 1 In this trial, patients were recruited if they had low LDL-C values but elevations in hs-CRP. It was a double-blind, placebo-controlled, multi-center, event-driven, primary prevention trial of over 17,000 men and women . . . and it was stopped over two years early because of the tremendous efficacy that rosuvastatin (Crestor) showed in lowering CV events (even in “low-risk” patients). In this trial, patients with normal LDL cholesterol but positive inflammation (indicated by hs-CRP), had worsening atherosclerosis (as measured by CIMT). The only patients who experienced plaque regression were the ones who controlled both cholesterol and inflammation.
Many other well-designed studies have confirmed CV risk associated with elevations in CRP. The Women’s Health Study that included over 27,000 “apparently healthy” middle-aged women, showed that CRP was actually better than LDL cholesterol for predicting CV risk in women. 5 In addition, the Harvard-sponsored Physicians' Health Study of around 21,000 men demonstrated that CRP could predict heart disease before it was otherwise evident. 6 And in the AFCAPS/TexCAPS study (Air Force/Texas Coronary Atherosclerosis Prevention Study), individuals with below-median LDL and above-median CRP levels had a similar risk of future vascular events as those with overt hyperlipidemia. 4
So clearly the problem is not just cholesterol - vascular inflammation needs to be identified and treated in order to lower CV risk in patients.
In response to the convincing data from the JUPITER trial, the American Heart Association and the American College of Cardiology now recommend measuring CRP in men 50 years of age or older or women 60 years of age who have normal LDL cholesterol (< 130 mg/dL). Knowing this information can help clinicians determine which patients may still benefit from statin cholesterol medication. 3
C-reactive protein is an acute phase inflammatory plasma protein made by the liver, so it will rise in conjunction with systemic inflammation from many different sources. For this reason, the “high sensitivity” CRP test is necessary for detecting low levels of CRP that correlate more with endothelial (vascular) inflammation.
In general, if “high sensitivity” CRP is between 1-5 then it is more likely a marker of CV risk, but if it is over 10 then the elevation could be from an acute infection, a recent injury, or another non-cardiac source like autoimmune disease.
The hs-CRP biomarker should decline with effective disease management, so it can also provide independent prognostic information after initiating treatment (to help assess how well a patient is responding to lifestyle changes and statin medication).
We cannot discuss hs-CRP without acknowledging the results of the Jupiter Trial. 1 In this trial, patients were recruited if they had low LDL-C values but elevations in hs-CRP. It was a double-blind, placebo-controlled, multi-center, event-driven, primary prevention trial of over 17,000 men and women . . . and it was stopped over two years early because of the tremendous efficacy that rosuvastatin (Crestor) showed in lowering CV events (even in “low-risk” patients). In this trial, patients with normal LDL cholesterol but positive inflammation (indicated by hs-CRP), had worsening atherosclerosis (as measured by CIMT). The only patients who experienced plaque regression were the ones who controlled both cholesterol and inflammation.
Many other well-designed studies have confirmed CV risk associated with elevations in CRP. The Women’s Health Study that included over 27,000 “apparently healthy” middle-aged women, showed that CRP was actually better than LDL cholesterol for predicting CV risk in women. 5 In addition, the Harvard-sponsored Physicians' Health Study of around 21,000 men demonstrated that CRP could predict heart disease before it was otherwise evident. 6 And in the AFCAPS/TexCAPS study (Air Force/Texas Coronary Atherosclerosis Prevention Study), individuals with below-median LDL and above-median CRP levels had a similar risk of future vascular events as those with overt hyperlipidemia. 4
So clearly the problem is not just cholesterol - vascular inflammation needs to be identified and treated in order to lower CV risk in patients.
In response to the convincing data from the JUPITER trial, the American Heart Association and the American College of Cardiology now recommend measuring CRP in men 50 years of age or older or women 60 years of age who have normal LDL cholesterol (< 130 mg/dL). Knowing this information can help clinicians determine which patients may still benefit from statin cholesterol medication. 3

b) Lp-PLA2 (lipoprotein-associated phospholipase A2)
This test will determine if your arteries are "on fire." Lp-PLA2 is an enzyme marker of plaque forming, cracking, or shifting . . . but unlike hsCRP, Lp-PLA2 is vascular-specific (and is not affected by smoking). 8 Due to its pro-inflammatory and pro-oxidative effects, Lp-PLA2 plays a key role in the pathogenesis of atherosclerosis (plaque build up in the arteries). It is localized in the necrotic lipid core of the plaque (below the collagen or calcified cap) so it is associated with soft, active, rupture-prone plaque (as opposed to stable calcified plaque).
Lp-PLA2 is produced by inflammatory cells (macrophages, T-cells, and mast cells) and is primarily bound to LDL cholesterol. The Lp-PLA2 enzyme plays a role in the oxidation of these LDL particles into atherogenic substances. 2 These substances are known triggers in the inflammatory cascade, and they accumulate in the intimal wall (inner lining of the artery). This leads to the development of foam cells, which in turn progresses into fatty streaks (the first sign of atherosclerosis). 5
A meta-analysis involving a total of 79,036 participants in 32 prospective studies found that Lp-PLA2 levels are positively correlated with the risk of developing coronary heart disease and stroke. 3 This increased risk of cardiovascular (CV) disease is independent of LDL-C and other inflammatory markers. 7
According to the ARIC trial, the stroke risk goes up from 2-fold to 11-fold when hsCRP is also elevated. 6 And when Lp-PLA2 is elevated in conjunction with systolic blood pressure, the patient has a 7-fold increased risk of a CV event or stroke.
LpPLA2 is now included in four major international society guidelines: 5
The American College of Cardiology, the American Heart Association, the American Association of Clinical Endocrinologists, and the European Society of Cardiology all agree that measurement of Lp-PLA2 activity is useful for risk stratification of asymptomatic adult patients. 5
This test will determine if your arteries are "on fire." Lp-PLA2 is an enzyme marker of plaque forming, cracking, or shifting . . . but unlike hsCRP, Lp-PLA2 is vascular-specific (and is not affected by smoking). 8 Due to its pro-inflammatory and pro-oxidative effects, Lp-PLA2 plays a key role in the pathogenesis of atherosclerosis (plaque build up in the arteries). It is localized in the necrotic lipid core of the plaque (below the collagen or calcified cap) so it is associated with soft, active, rupture-prone plaque (as opposed to stable calcified plaque).
Lp-PLA2 is produced by inflammatory cells (macrophages, T-cells, and mast cells) and is primarily bound to LDL cholesterol. The Lp-PLA2 enzyme plays a role in the oxidation of these LDL particles into atherogenic substances. 2 These substances are known triggers in the inflammatory cascade, and they accumulate in the intimal wall (inner lining of the artery). This leads to the development of foam cells, which in turn progresses into fatty streaks (the first sign of atherosclerosis). 5
A meta-analysis involving a total of 79,036 participants in 32 prospective studies found that Lp-PLA2 levels are positively correlated with the risk of developing coronary heart disease and stroke. 3 This increased risk of cardiovascular (CV) disease is independent of LDL-C and other inflammatory markers. 7
According to the ARIC trial, the stroke risk goes up from 2-fold to 11-fold when hsCRP is also elevated. 6 And when Lp-PLA2 is elevated in conjunction with systolic blood pressure, the patient has a 7-fold increased risk of a CV event or stroke.
LpPLA2 is now included in four major international society guidelines: 5
The American College of Cardiology, the American Heart Association, the American Association of Clinical Endocrinologists, and the European Society of Cardiology all agree that measurement of Lp-PLA2 activity is useful for risk stratification of asymptomatic adult patients. 5
c) MPO (Myeloperoxidase)
Myeloperoxidase is a vascular specific enzyme that is a marker and mediator of inflammation and oxidative stress. It can be an indicator of plaque forming or breaking. This test can help determine if you are at risk of a plaque rupture (that can cause a sudden heart attack or stroke).
White blood cells release MPO when an arterial wall is inflamed or damaged (from the luminal side of the plaque), so elevated levels may indicate the presence of unstable plaque (which can suddenly rupture and cause a heart attack or stroke). In addition, MPO oxidatively modifies LDL cholesterol, as well as causing HDL to be less functional . . . which both precipitate atherogenesis by leading to an excess of cholesterol rich plaque in the arterial wall. 2
“Multiple lines of evidence suggest an association between MPO and cardiovascular disease including coronary artery disease, congestive heart failure, arterial hypertension, pulmonary arterial hypertension, peripheral arterial disease, myocardial ischemia/reperfusion-related injury, stroke, cardiac arrhythmia and venous thrombosis.” 4 “In addition, plasma and serum levels of MPO have been shown to predict risks of subsequent major adverse cardiac events (nonfatal myocardial infarction, death, and need for revascularization) in patients presenting with either chest pain or acute coronary syndromes.” 3
Overall, elevated MPO levels are associated with a poor prognosis. 4 Thus in patients with high levels of MPO, careful evaluation of cardiovascular risk should be considered by the healthcare professional so appropriate interventions can be implemented to lower MPO and subsequent CV risk.
Myeloperoxidase is a vascular specific enzyme that is a marker and mediator of inflammation and oxidative stress. It can be an indicator of plaque forming or breaking. This test can help determine if you are at risk of a plaque rupture (that can cause a sudden heart attack or stroke).
White blood cells release MPO when an arterial wall is inflamed or damaged (from the luminal side of the plaque), so elevated levels may indicate the presence of unstable plaque (which can suddenly rupture and cause a heart attack or stroke). In addition, MPO oxidatively modifies LDL cholesterol, as well as causing HDL to be less functional . . . which both precipitate atherogenesis by leading to an excess of cholesterol rich plaque in the arterial wall. 2
“Multiple lines of evidence suggest an association between MPO and cardiovascular disease including coronary artery disease, congestive heart failure, arterial hypertension, pulmonary arterial hypertension, peripheral arterial disease, myocardial ischemia/reperfusion-related injury, stroke, cardiac arrhythmia and venous thrombosis.” 4 “In addition, plasma and serum levels of MPO have been shown to predict risks of subsequent major adverse cardiac events (nonfatal myocardial infarction, death, and need for revascularization) in patients presenting with either chest pain or acute coronary syndromes.” 3
Overall, elevated MPO levels are associated with a poor prognosis. 4 Thus in patients with high levels of MPO, careful evaluation of cardiovascular risk should be considered by the healthcare professional so appropriate interventions can be implemented to lower MPO and subsequent CV risk.
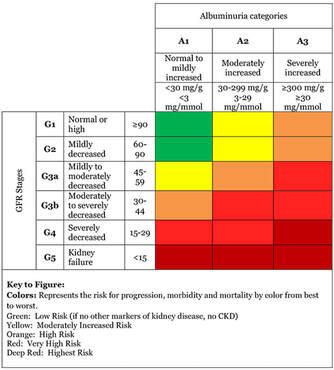
d) Urine microalbumin/creatinine ratio
The urine microalbumin-creatinine ratio shows whether you have albumin in your urine. Albumin is a type of protein that's normally found in the blood.
If kidneys are healthy, they should let only very little protein go into your urine – or even none. But if your kidneys are damaged, protein can "leak" out of the kidneys into your urine. People with a high amount of albumin in their urine are at an increased risk of having chronic kidney disease (CKD) progress to kidney failure.
A normal amount of albumin in your urine is less than 30 mg/g. Anything above 30 mg/g may mean you have kidney disease, even if your estimated glomerular filtration (eGFR) number is above 60.
How can you protect your kidney function?
- Control blood pressure if you have high blood pressure.
- Control blood sugar if you have diabetes.
- In general, if you have CKD, avoid non-steroidal anti-inflammatory drugs (NSAIDs) such as ibuprofen and naproxen.
- If you have CKD, tell your healthcare team before having any test that uses contrast dye.
- Do not smoke.
- Exercise and follow a healthy diet that's low in sodium, saturated fat, and sugar, but high in fresh fruits, vegetables, whole grains, lean meats, fish, and poultry. Avoid highly processed foods.
- Stay at a healthy weight. Lose weight if your healthcare team says that you should.
- Discuss any vitamins, minerals, herbs, weight loss or body building supplements with your healthcare team before taking them. Many of these products can hurt your kidneys.
- Make sure that any drugs you take are the right dose for your age and your level of kidney function. You should discuss this with your healthcare team.
REFERENCES
1 – El Harchaoui, et. al. (2007). Value of Low-Density Lipoprotein Particle Number and Size as Predictors of Coronary Artery Disease in Apparently Healthy Men and Women: The EPIC-Norfolk Prospective Population Study. J Am Coll Cardiol, 49(5), 547-553.
2 – Mora, S., et. al. (2015). Atherogenic Lipoprotein Subfractions Determined by Ion Mobility and First Cardiovascular Events After Random Allocation to High-Intensity Statin or Placebo: The JUPITER Trial. Circulation. Doi:10.1161/circulationaha.115.016857
3 - Wilkins, J. T., et. al. (2016). Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification The CARDIA Study. J Am Coll Cardiol, 67(2), 193-201.
4 – Rosenson, R. S., Hegele, R. A., & Gotto, J. A. M. (2016). Integrated Measure for Atherogenic Lipoproteins in the Modern Era Risk Assessment Based on Apolipoprotein B. J Am Coll Cardiol, 67(2), 202 – 204.
5 – Circulation. 2000;101:477-484; Gotto, et. al.
6 – Lancet. 2003;361:777-780; Sniderman
7 - https://www.ncbi.nlm.nih.gov/pubmed/21487090
8 - https://www.aarp.org/health/healthy-living/info-2018/bob-harper-heart-attack-fd.html
9 – https://www.ncbi.nlm.nih.gov/pubmed/19081406
10 - https://www.ncbi.nlm.nih.gov/pubmed/11755609
11 - https://www.ncbi.nlm.nih.gov/pubmed/16316964
12 - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC80634/
13 - https://www.ahajournals.org/doi/10.1161/hc1002.105136
14 – Superko HR. Beyond LDL-C, Circ. 1996;94:2351-2354
15 – Akosah KO, Schaper A, Cogbill C. J Am Coll Cardiol. 2003;41(9):1475-1479.
16 – Berman et al. J Am Coll Cardiol. 2004;44:923-30.
17 – Grundy SM, et al. Circulation. 2005; 112:2735-2752
18 – Pearson TA et al, Circulation 2003;107:499-511
19 – Hlatky MA et al. Circulation 2009;119:2408-2416 3. Greenland P et al. Circulation 2007;115:402-426
20 – Greenland P et al. Circulation 2010;122:e584-e636
21 - https://www.healthline.com/health/heart-disease/statistics
22 - https://www.mayoclinicproceedings.org/article/S0025-6196(14)00800-3/pdf
23 - https://www.nejm.org/doi/full/10.1056/NEJMoa0807646
24 - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3165136/
25 - https://www.ncbi.nlm.nih.gov/pubmed/17645591
Whole Heart Family Medicine
National Kidney Foundation
1 – El Harchaoui, et. al. (2007). Value of Low-Density Lipoprotein Particle Number and Size as Predictors of Coronary Artery Disease in Apparently Healthy Men and Women: The EPIC-Norfolk Prospective Population Study. J Am Coll Cardiol, 49(5), 547-553.
2 – Mora, S., et. al. (2015). Atherogenic Lipoprotein Subfractions Determined by Ion Mobility and First Cardiovascular Events After Random Allocation to High-Intensity Statin or Placebo: The JUPITER Trial. Circulation. Doi:10.1161/circulationaha.115.016857
3 - Wilkins, J. T., et. al. (2016). Discordance Between Apolipoprotein B and LDL-Cholesterol in Young Adults Predicts Coronary Artery Calcification The CARDIA Study. J Am Coll Cardiol, 67(2), 193-201.
4 – Rosenson, R. S., Hegele, R. A., & Gotto, J. A. M. (2016). Integrated Measure for Atherogenic Lipoproteins in the Modern Era Risk Assessment Based on Apolipoprotein B. J Am Coll Cardiol, 67(2), 202 – 204.
5 – Circulation. 2000;101:477-484; Gotto, et. al.
6 – Lancet. 2003;361:777-780; Sniderman
7 - https://www.ncbi.nlm.nih.gov/pubmed/21487090
8 - https://www.aarp.org/health/healthy-living/info-2018/bob-harper-heart-attack-fd.html
9 – https://www.ncbi.nlm.nih.gov/pubmed/19081406
10 - https://www.ncbi.nlm.nih.gov/pubmed/11755609
11 - https://www.ncbi.nlm.nih.gov/pubmed/16316964
12 - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC80634/
13 - https://www.ahajournals.org/doi/10.1161/hc1002.105136
14 – Superko HR. Beyond LDL-C, Circ. 1996;94:2351-2354
15 – Akosah KO, Schaper A, Cogbill C. J Am Coll Cardiol. 2003;41(9):1475-1479.
16 – Berman et al. J Am Coll Cardiol. 2004;44:923-30.
17 – Grundy SM, et al. Circulation. 2005; 112:2735-2752
18 – Pearson TA et al, Circulation 2003;107:499-511
19 – Hlatky MA et al. Circulation 2009;119:2408-2416 3. Greenland P et al. Circulation 2007;115:402-426
20 – Greenland P et al. Circulation 2010;122:e584-e636
21 - https://www.healthline.com/health/heart-disease/statistics
22 - https://www.mayoclinicproceedings.org/article/S0025-6196(14)00800-3/pdf
23 - https://www.nejm.org/doi/full/10.1056/NEJMoa0807646
24 - https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3165136/
25 - https://www.ncbi.nlm.nih.gov/pubmed/17645591
Whole Heart Family Medicine
National Kidney Foundation